Abstract
Hepatitis C virus (HCV) is a key RNA virus that contributes in the progressive damage of the liver. HCV infections have been shown to progress and eventually initiate the onset of complications such as cirrhosis and liver cancer. It is projected that close to 100 million individuals worldwide suffer from HCV infections. Recent statistics have shown that HC is the major predisposing factor for liver transplantation in most countries worldwide. Following the detection of HCV in 1989, research activities have led to the identification of novel and improved diagnostic tools as well as management strategies. Over the past few years, targeted drugs referred to as direct-acting antiviral agents (DAA)-based regimens have been produced to aid in treating and managing HCV infection. As opposed to the use of the previous interferon (IFN)-based therapies, DAA therapy produces significant beneficial health effects including enhancing the quality of life of HC patients various DAA agents such as simeprevir and sofosbuvir have been authorized for pharmaceutical use in the treatment HCV GT4. However, there are very few studies that have investigated the effectiveness and safety of DAA agents in patients suffering from for HCV. This research paper has effectively discussed the various aspects of HCV including its incidence, modes of transmission, its life cycle, pathogenesis, and the current preventive measures for HCV. This research paper has also analysed the study conducted by El Raziky et al. (2017) in order to understand the contribution of simeprevir and sofosbuvir in managing HCV GT4. The outcomes of this study support previous findings which showed that simeprevir and sofosbuvir are highly effective and well-tolerated drug therapies for HCV GT4.
Key words: Hepatitis C virus, Simeprevir, Sofosbuvir, Genotype 4, Virions
Save your time!
We can take care of your essay
- Proper editing and formatting
- Free revision, title page, and bibliography
- Flexible prices and money-back guarantee
Background
Hepatitis C infection is an illness that affects the liver. This illness is initiated by HCV occurring in the blood of individuals possessing the disease. HCV is a spherical enveloped and positive strand ribonucleic acid (RNA) virus. HCV infection has been shown to cause acute hepatitis C infection, with close to 60% of the affected people developing chronic hepatitis C (Manns et al., 2017). HCV is responsible for causing hepatitis C through two main ways. The first means is by infecting the cell. It then kills the cell or damages it. This method of disease infection is referred to as cytopathic damage. The second means of HCV infection is through provocation of the immune response. A misdirected or overactive immune response has the potential to damage the infected cells as well as the surrounding tissues. This method of HCV infection is referred to as immunopathic damage (Razavi et al., 2014).
There are various signs and symptoms associated with HCV infection with the generalized symptoms being pain of the joints, fatigue, fever, myalgia, weakness and sleep disturbances. The pain reported in the joints of individuals with HCV infection is referred to as arthralgia. The common joints that suffer pain include the hips, knees, spine and fingers. The joint pain associated with hepatitis C is migratory, with the discomfort moving from one part of the body to another. Individuals with hepatitis C are also reported to experience fatigue which may be mild or severe. Individuals with hepatitis C often experience fever. As the fever reduces, some of the patients may experience chills and night sweating. Apart from the pain of the joints, individuals suffering from hepatitis C can suffer from muscle pain, also referred to as myalgia. Myalgia symptom appear intermittently and do not last long. Patients suffering from hepatitis C can sometimes experience a general sense of weakness. Further, they may suffer sleep disturbances, and in most cases may stake awake during the night. All these are subjective evidences of hepatitis C (Yuen et al., 2018).
The objective evidences include; cognitive changes, depression, blood sugar abnormalities, and ascites. Some individuals with hepatitis C may experience changes in their cognitive ability with most of the individuals finding it difficult to concentrate for long periods of time. In addition, the though process tends to become slower. Hepatitis C is responsible for causing depression indirectly by bringing changes that lead to depression such as irritability, sleep disturbances, and a sense of hopelessness. Another key feature of hepatitis C is that it has the ability to induce blood sugar imbalance in the body. High levels of blood sugar causes individuals to experience symptoms such as fatigue, thirst, frequent urination, and weight loss. Low blood sugar on the other hand causes individuals to suffer nausea, dizziness, weakness and light-headedness (Pfaender et al., 2015).
There are various complications linked with HC including cirrhosis, liver failure, and liver cancer. Liver cirrhosis is the commonly occurring complication. In such a case, the liver develops a scarred tissue that replaces the healthy tissue and eventually prevents the liver form functioning effectively. As a result of liver cirrhosis, the liver may lose its functions completely causing the affected individuals to suffer end-stage liver disease or liver failure. Another complication of hepatitis that has been on the rise in the past few decades is liver cancer. It is estimated that approximately 1 in 20 people suffering from hepatitis associated with cirrhosis eventually develop liver cancer (Reig et al., 2016). Unfortunately, there has been no successful cure for liver cancer.
HCV is transmitted mainly through exposure of the blood or body fluids containing the virus to individuals who are not infected. Infection can occur following the sharing of items such as tooth brushes, razor blades, diabetic lancelets and needles. Transmission of HCV can also occur via sexual and mother-to-mother transmission. The incidence of chronic HCV infection is considered to be approximately 1.7% in the adult global population, indicating that more than 75 million individuals are affected by the illness. Based on a recent survey, it is projected that the prevalence of HCV infection was about 3.5 million in the US (Messina et al., 2015). The occurrence of HCV infection varies considerably across nations worldwide, with the highest rates of infection occurring in countries with a history of iatrogenic infections (infections associated with medical therapy). The infection was reported to occur mostly in Africa and the Middle East countries such as Egypt, Cameroon, Mongolia, Uzbekistan, and Nigeria. The population infected by HCV has a peak age of about 30-35 years, but a higher peak age of approximately 50 to 60 years has been reported in countries dominated by iatrogenic infections (Blach et al., 2017).
The RNA of HCV can be traced in the blood, saliva, seminal fluid, tears, and cerebrospinal fluid. For majority of the affected individuals in the US and Europe, the HCV infection is obtained through intravenous drug abuse. Studies have shown that there exist various HCV genotypes that are based on variability of the nucleotide in HCV sequences obtained from diverse geographical regions; genotype 1 has the highest dispersal globally. Approximately 70% of isolates obtained from the US are subtype 1a and 1b; genotype 2 has been shown to be widely distributed in central and west Africa; genotype 3 is diverse in Asia; genotype 4 on the other is prevalent in Africa and the Middle East; genotypes 5 and 7 occur in Africa while genotype 6 occurs predominantly in Southeast Asia (Mohd Hanafiah et al., 2013).
HCV belongs to the family Flaviviridae and genus Hepacivirus. The HCV virions have a diameter of approximately 50 to 60 nm and are covered by a lipid bilayer that anchors two gylycoproteins (E1 and E2). The genome is about 9.6 kb in length. Hepatitis C is considered to be a key public health concern in various parts of the world including the United States. The HCV RNA genome can interact with the primary protein resulting in the formation of viral nucleocapsid and cytosolic lipid droplets. The nucleocapsid is covered by a lipid-rich cover and contains E1 and E2 glycoprteins that facilitate the entry of the virus through receptor binding and fusion. The E1 and E2 glycoproteins have the ability to create non-covalent heterodimers with the infected cells. The HCV virion can associate with other types of lipoproteins including apoB, apoE, apoC1, apoC2 to generate a complex lipoviroparticle (LVP) that can influence the entry of HCV (Pybus & Thézé. 2016).
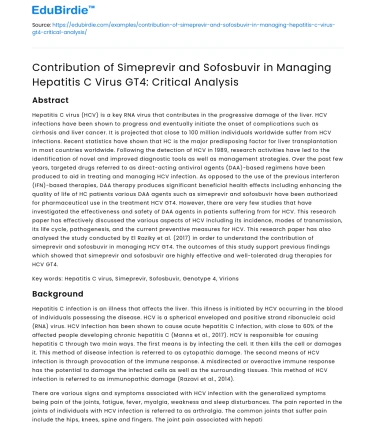
Stages of the HCV life cycle
The first stage of the HCV lifecycle involves virion attachment to the receptors on hepatocyctes. The cellular receptors that initiate the attachment step of HCV lifecycle include high-density lipoprotein receptor, scavenger receptor class B, occluding, tetraspanin CD81, and tight junction protein claudin-1. During this stage, the virus binds with the receptor complex and after internalization, the nucleocapsid moves out into the cytoplasm (Scheel & Rice, 2013).
The second stage involves uncoating where the genomic RNA is released into the cytosol as shown in the figure below, where is functions as mRNA for the production of HVC polyprotein.
Figure: Illustration of the stage of the HCV life cycle (Dustin, Bartolini, Capobianchi & Pistello, 2016)
The large polyprotein that is produced undergoes translation in the endoplasmic reticulum. This results in the formation of three structural and seven unstructured proteins. After processing, the proteins are still attached with the intracellular membranes.
The next stage is the replication which is catalyzed by the NS5B protein. During the virus replication phase, the NS5A protein and helicase-NTPase regions of the NS3 play a regulatory role. The NS5A protein serves as a dimer involved RNA binding. The two domains (I and II) found in the NS5A protein have some key roles in the HCV replication. The NS3 helicase is involved in enhancing the separation of original and template strands of RNA. The NTPase/helicase part of the NS3 protein has various roles that are necessary for replication such as RNA binding, RNS induced NTPase activity, and opening up of the RNA regions of the entire secondary structure. The NS4B induces the generation of the replication complex that facilitates replication of HCV. Additionally, the NS5A protein contributes in enhancing regulation of the virus replication. Following the replication process, new direct acting antivirals (DAAs) are made available (Afzal et al., 2015).
In the next two stages, the virions are aggregated in an endoplasmic reticulum-derived section and are subsequently released through exocytosis. Along the process, the virus becomes mature and is encircled by lipoproteins that facilitate immune escape (Li & Lo, 2015).
Pathogenesis of HCV infection
The HC RNA virus moves into the hepatocyte through endocytosis with the process being mediated by four co-receptor molecules. The HC RNA virus is internalized in the cytoplasm and thereafter, the positive-stranded RNA is uncoated and translated into 10 mature peptides. The peptides are cleaved by the host proteases as well as by the virally encoded proteases referred to as NS3-4a serine proteases. Following the cleavage process, the mature peptides move and reside on the ER. This results in the generation of a replication molecule that contains a critical enzyme known as the NS5B RNA dependent RNA polymerase which catalyzes the positive strand of the RNA to form an intermediate with a negative strand. The intermediate can be utilized as a template for the synthesis of a new positive strand. The RNAs are packaged with the essential envelope glycoprotein into mature virions. The virions subsequently the cell via exocytosis. Within one to four weeks of exposure, the virus can be identified in the plasma. Viremia has been shown to peak in approximately 8 to 12 weeks after infection. Thereafter if plateaus or declines to undetectable levels in a process known as viral clearance. Continued and sustained infection is associated with the weak CD4+ and CD8+ T cell responses that are not effective in controlling viral replication (Irshad, Mankotia & Irshad, 2013).
How the host’s body fights infection
Immediately after initiating infection in the hepatic centers, the HCV goes through replication to generate more viruses. However, the replication is slowed down abruptly when the liver cells express various IFN-stimulated genes (ISGs) that prevent the replication of HCV. Innate immunity acts as the first line of defense against the infection caused by HC virus. Innate immunity contributes in stimulating adaptive immunity (Honer & Gale Jr. 2013). The HCV RNA becomes attached to the retinoic acid-inducible gene I and in the process activate the mitochondrial antiviral signaling (MAVS) proteins. The RNA that is bound to the Toll-like receptor-3 stimulates the initiation of signaling through the TRIF. The two pathways activate the translocation of NFκB and IRF3 to the nucleus. In the process, they stimulate the expression of ISGs and IFNs to prevent further viral replication. They also stimulate the proinflammatory cytokines as well as chemokines to activate the immune cells. The NS3-4A protease of the HCV cleaves TRIF and MAVS so to limit the induction of IFN. Hepatocytes have also been shown to induce IFN-λ after HCV infection. In addition, Kupffer cells, dendritic cells and other non-parenchymal cells start to recognize the molecular patterns of viruses and contribute to the generation of IFN and cytokines without themselves being infected by the replicating HCV (Boljes et al., 2014).
Current preventive measures of HCV
According to the World Health Organization (WHO), the preventive measures for HCV infection can be categorized into primary and secondary prevention measures. The primary measures include screening and testing of blood, plasma and other biological samples (He et al., 2016). It also includes the inactivation of virus in plasma-derived products. Other important activities include the implementation of counselling services to reduce risk as well as the implementation and maintenance of practices that control HCV infection. Secondary prevention measures include the identification and provision of counselling and testing services to individuals at risk. Moreover, it involves the medical management of people infected with HCV.
Purpose of the study and hypothesis
This research was carried out to examine the safety and effectiveness of a combinational of simeprevir and sofosbuvir in treating individuals with or without cirrhosis.
The hypothesis was that a combination of simeprevir (150 mg) and sofosbuvir (400 mg) given to HCV genotype 4 patients with or without cirrhosis daily for a period of eight to 12 weeks was safe and effective in managing HCV.
Independent and dependent variables
Independent variables are the dosage of the two drugs (simeprevir (150 mg) and sofosbuvir (400 mg) and the frequency of administration of the drugs. The independent variable is one that is manipulated by the researcher.
The dependent variables in the study are efficacy, safety and tolerability. These are the outcome variables that were measured at the various time intervals. Efficacy, safety, and tolerability were the outcomes measured so as to determine the findings of the experiment.
The control variables were the Peg-IFN/RBV control rates. This was a positive control, and it was considered as the standard of care for the treatment of HCV during the period in which the study was designed. The controlled variables are a standard measure used to compare the results of an experiment. In this case the previous results obtained using Peg-IFN/RBV will be used to make comparisons with the results from this study.
Study design
Figure: A flow diagram showing the experimental design
The study was conducted in three different sites in Egypt. The inclusion required that participants be aged between 18 and 70 years. Participants with experience in Peg-IFN/RBV were included in the research. Patients with liver disease but no HCV aetiology were excluded from the study. Moreover, individuals co-infected or infected with non-GT4 HCV were not included in the study. After providing consent to participate in the study, the participants in groups A2 and B were tested at baseline for plasma HCV. Participants were allocated into two major groups; Group A comprised of patients without cirrhosis. They were randomized in a ratio of 1:1 and placed into an 8-week treatment group (Group A1) or a 12-week treatment group (Group 12). Participants with cirrhosis were placed in Group B where they received treatment for 12 weeks as illustrated in the figure above. Baseline data was also obtained at weeks 1, 2, 4, 8, and 12. The study evaluations conducted for each group at the end of the treatment process included efficacy assessments and safety evaluations.
Results
From the study, it was observed that the sustained response after 12 weeks of treatment was approximately 92% (95% CI) as observed in the table below. This value was significantly higher compared that of the historical control rate which was 42%. This demonstrated the effectiveness of the treatment regimen in comparison with the historical treatment.
Treatment group General SVR12 rate 95% CI Historical control (SVR rate)
- All patients 58/63 (92%) 82.4, 97 41
- Noncirrhotic patients (8 weeks) 15/20 (75%) 50.9, 91 50
- Noncirrhotic patients (12 weeks) 20/20 (100%) 83.2, 100 50
- Noncirrhotic patients (8&12 weeks) 35/40 (88%) 73.1, 96 50
- Cirrhotic patients (12 weeks) 23/23 (100%) 85.1, 100 26
Table: The comparison of SVR12 treatment rates with historical control rates (El Raziky et al., 2017)
Eight weeks of treatment produced an SVR12 rate of 75% while the participants in treatment Group A2 experienced an SVR12 rate of 100%.
Further, after eight weeks of treatment, 100% of the participants had undetectable HCV RNA. All the participants under treatment for the 12 weeks exhibited sustained virologic response. In addition, all the participants who managed to achieve SVR4 were observed to SVR12 and SVR24.
With regards to virologic failure, no patient was reported to experience on-treatment failure. Of the 81% of the participants who experienced treatment emergent adverse effects, only 30% reported adverse events that were considered to be associated with simeprevir and sofosbuvir. Most of the adverse events were categorized as Grade 1 or 2. Only 3% of the patients were reported to experience Grade 3 adverse events, with a similar trend reported in Grade 4 adverse events (only 3% of patients affected). The adverse events that were reported in more than 5% of the patients and which were indicated to be associated with simeprevir were headache (13%), pruritis (11%) and fatigue (8%) as shown in the table below.
Common adverse events associated with simeprivir
- Group A1 (n=20) Group A2 (n=20) Group B (n=23) All (n=63)
- Headache 2 (10) 1 (5) 5 (22) 8 (13)
- Pruritis 3 (15) 1 (5) 3 (13) 7 (11)
- fatigue 1 (5) 3 (15) 1 (4) 5 (8)
Occurrence of more than 1 adverse events 80% 65% 96% 81%
Table: adverse effects associated with simeprivir (El Raziky et al., 2017).
Major finding of the study
The key finding of this study was that the results were consistent with recent studies conducted in other parts of the world, particularly with regards to individuals infected with HCV GT4. In conclusion it was found that combination of simeprevir and sofosbuvir administered for 12 weeks was highly effective and well-tolerated by patients with HVC GY4.
Importance of the study findings
Given that only a few studies have been carried out to examine the use of simeprevir-based regimens in the treatment of HCV GT4, the findings from this study will be useful in providing more information about the safety and effectiveness of this therapy in the health care setting. This is beneficial to medical practitioners, because they have additional source of information that will help influence their choice of treatment.
Limitations
The participants used in the study was not relatively small and thus the outcome of this study may not be generalizable. The partly randomized design of the study was reported to be a limiting factor because it prevents the drawing of comparisons between cirrhotic and non-cirrhotic patients.
The study focused on the key aspects of drugs that inform the choice of medical practitioners whether to adopt or ban the use of specific drugs. Effectiveness and safety can shape the quality of life of individuals using the specific drugs.
Factor contributing to the impact of hepatitis C in the society
Key factors such as recipient, donor, or transplant-related factors have been reported to contribute to the impact of HC among individuals in the society. With regards to donor factor, the old age of a donor has been linked with progressive HCV illness and graft loss in some cases. According to Gambato et al. (2014), there exists a 65% higher likelihood of graft loss among old donors aged between 40-50 years old. However, the likelihood increases to about 86% for donors aged between 50 and 60 years. The rate is significantly higher (221%) for donors who are above 60 years old. Therefore, it is highly discouraged to use elderly donors. It can thus be noted that old age plays a significant role in the recurrence or progression of HCV infection in individuals receiving transplants (Younossi etal., 2014).
References
- Afzal, M. S., Alsaleh, K., Farhat, R., Belouzard, S., Danneels, A., Descamps, V. ... & Rouillé, Y. (2015). Regulation of core expression during the hepatitis C virus life cycle. Journal of General Virology, 96(2), 311-321.
- Blach, S., Zeuzem, S., Manns, M., Altraif, I., Duberg, A. S., Muljono, D. H. ... & Abaalkhail, F. (2017). Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. The Lancet Gastroenterology & Hepatology, 2(3), 161-176.
- Boltjes, A., Movita, D., Boonstra, A., & Woltman, A. M. (2014). The role of Kupffer cells in hepatitis B and hepatitis C virus infections. Journal of Hepatology, 61(3), 660-671.
- Dustin, L. B., Bartolini, B., Capobianchi, M. R., & Pistello, M. (2016). Hepatitis C virus: life cycle in cells, infection and host response, and analysis of molecular markers influencing the outcome of infection and response to therapy. Clinical Microbiology and Infection, 22(10), 826-832.
- El Raziky, M., Gamil, M., Ashour, M. K., Sameea, E. A., Doss, W., Hamada, Y. ... & Hammad, R. (2017). Simeprevir plus sofosbuvir for eight or 12 weeks in treatment‐naïve and treatment‐experienced hepatitis C virus genotype 4 patients with or without cirrhosis. Journal of Viral Hepatitis, 24(2), 102-110.
- Gambato, M., Lens, S., Fernández-Carrillo, C., Alfaro, I., & Forns, X. (2014). Viral hepatitis and liver transplantation: pathogenesis, prevention and therapy of recurrent disease. Digestive Diseases, 32(5), 538-544.
- He, T., Li, K., Roberts, M. S., Spaulding, A. C., Ayer, T., Grefenstette, J. J., & Chhatwal, J. (2016). Prevention of hepatitis C by screening and treatment in US prisons. Annals of Internal Medicine, 164(2), 84-92.
- Horner, S. M., & Gale Jr, M. (2013). Regulation of hepatic innate immunity by hepatitis C virus. Nature Medicine, 19(7), 879.
- Irshad, M., Mankotia, D. S., & Irshad, K. (2013). An insight into the diagnosis and pathogenesis of hepatitis C virus infection. World Journal of Gastroenterology: WJG, 19(44), 7896.
- Kim, C. W., & Chang, K. M. (2013). Hepatitis C virus: virology and life cycle. Clinical and Molecular Hepatology, 19(1), 17.
- Li, H. C., & Lo, S. Y. (2015). Hepatitis C virus: Virology, diagnosis and treatment. World Journal of Hepatology, 7(10), 1377.
- Manns, M. P., Buti, M., Gane, E., Pawlotsky, J. M., Razavi, H., Terrault, N., & Younossi, Z. (2017). Hepatitis C virus infection. Nature Reviews Disease Primers, 3, 17006.
- Messina, J. P., Humphreys, I., Flaxman, A., Brown, A., Cooke, G. S., Pybus, O. G., & Barnes, E. (2015). Global distribution and prevalence of hepatitis C virus genotypes. Hepatology, 61(1), 77-87.
- Mohd Hanafiah, K., Groeger, J., Flaxman, A. D., & Wiersma, S. T. (2013). Global epidemiology of hepatitis C virus infection: new estimates of age‐specific antibody to HCV seroprevalence. Hepatology, 57(4), 1333-1342.
- Pfaender, S., Cavalleri, J. M., Walter, S., Doerrbecker, J., Campana, B., Brown, R. J. ... & Baumgärtner, W. (2015). Clinical course of infection and viral tissue tropism of hepatitis C virus–like nonprimate hepaciviruses in horses. Hepatology, 61(2), 447-459.
- Pybus, O. G., & Thézé, J. (2016). Hepacivirus cross-species transmission and the origins of the hepatitis C virus. Current Opinion in Virology, 16, 1-7.
- Razavi, H., Waked, I., Sarrazin, C., Myers, R. P., Idilman, R., Calinas, F. ... & Akarca, U. (2014). The present and future disease burden of hepatitis C virus (HCV) infection with today's treatment paradigm. Journal of Viral Hepatitis, 21, 34-59.
- Reig, M., Mariño, Z., Perelló, C., Iñarrairaegui, M., Ribeiro, A., Lens, S. ... & Sangro, B. (2016). Unexpected early tumor recurrence in patients with hepatitis C virus-related hepatocellular carcinoma undergoing interferon-free therapy: a note of caution. Journal of Hepatology, 65(4), 719-26.
- Scheel, T. K., & Rice, C. M. (2013). Understanding the hepatitis C virus life cycle paves the way for highly effective therapies. Nature Medicine, 19(7), 837.
- Younossi, Z. M., Kanwal, F., Saab, S., Brown, K. A., El‐Serag, H. B., Kim, W. R. ... & Gordon, S. C. (2014). The impact of hepatitis C burden: an evidence‐based approach. Alimentary Pharmacology & Therapeutics, 39(5), 518-531.
- Yuen, M. F., Chen, D. S., Dusheiko, G. M., Janssen, H. L., Lau, D. T., Locarnini, S. A. ... & Lai, C. L. (2018). Hepatitis B virus infection. Nature R





 Stuck on your essay?
Stuck on your essay?

